
Youth Mental Health in Western North Carolina: Key Findings, Challenges, and Policy Solutions

Image Credit: Davis Evans via Unsplash
In 2023 and 2025, the North Carolina Child Health report card published by the North Carolina Institute of Medicine and NC Child gave the state a failing grade on youth mental health indicators, including high school students attempting suicide, mental health days reported by high school students, and access difficulties for mental health care for children ages 3-17.
Existing data shows that:
>50% of children reported struggling to access mental health treatment when needed (NCIOM & NC Child, 2025)
School-based health workforce is severely understaffed, with school psychologists operating at a 4x higher ratio of students to staff than recommended, while school social workers (4x), school nurses (2.5x) and school counselors (1.5x) were similarly overextended (ASCA, 2015; NASN, 2015; NCIOM & NC Child, 2025)
94 out of 100 counties in NC designated as mental health professional shortage areas (Susic & Ries, 2025)
Rural areas in North Carolina have roughly one-third to one-third the behavioral health workforce of urban counties (Woolcock et al., 2025)
So what does this mean for the state of mental health in Western North Carolina’s youth?
Youth Mental Health in WNC
In 2025, at the request of the WNC Healthy Impact Steering Committee, WNC Health Network (WNCHN) analyzed qualitative data from the 2024 WNC Healthy Impact Online Key Informant Survey[MA1] (unpublished report) to identify assets and barriers related to youth mental health in WNC.
📑 Full report of the analysis and other resources can be found on the WNCHN’s Youth Mental Health resources page.
On Friday, June 27th, 2026, WNCHN’s Meron Abebe (M.S., MBA, MPH), Director of Operations/ Evaluation & Learning Advisor, along with Emily Kujawa (MPH, RD), Director of Partner Engagement, joined WNC HPI partners to share findings from the analysis. The researchers shared data across five major themes shaping youth mental health in the region—access to care, care coordination and navigation, prevention and early intervention, youth engagement and supportive spaces, and social determinants of health—and invited feedback from providers, policymakers and others regarding their experiences and insights.
What we learned…
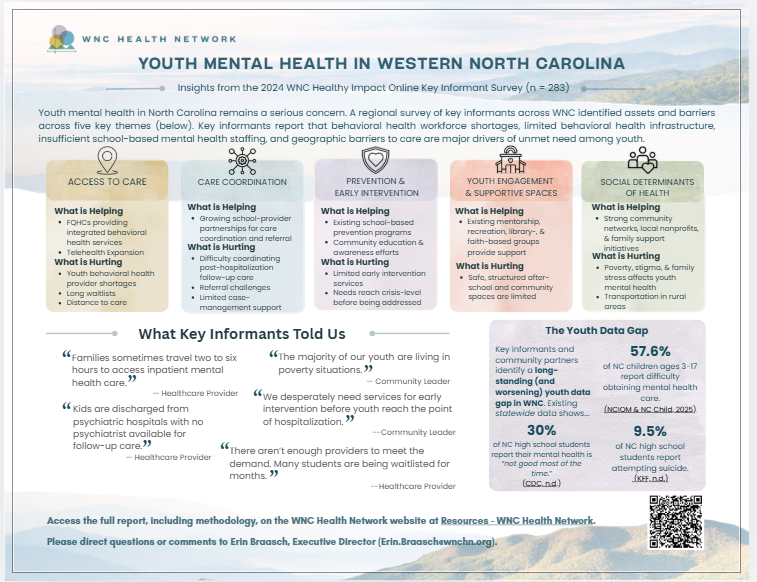
1-page summary of findings, courtesy of WNC Health Network. Available on their Youth Mental Health resources page.
Access to Care
Schools are expanding free or low-cost school-based services, tele-health is helping overcome transportation barriers, and Medicaid expansion has added some stability for families seeking care. These supports matter because many youth and families already interact with schools, primary care, and community organizations before they reach specialty behavioral health services.
However, challenges still exist. Provider participation and reimbursement challenges continue to limit access through Medicaid. Additionally, demand for youth mental health care continues to exceed capacity. Long waits, limited local crisis options, lack of referral options and follow up care, and provider shortages cause families to delay care or disengage from the system.
Finally, access should not be understood only as whether a network technically meets adequacy requirements. For families, access also means timely appointments, realistic travel distances, continuity of care, provider choice, and services that match a child’s level of need. Many families struggle to find, access, and retain ongoing access to a provider that works for them due to healthcare workforce shortages, travel challenges not related to distance, loss of services due to low utilization rates, challenges in finding providers that are contracted with their specific insurance plan or available at a time that works with their schedule, and other barriers.
Care Coordination and Navigation
There is a growing sense of collaboration between schools, healthcare providers, and community organizations. However, care transitions remain one of the weakest points in the youth mental health system, often breaking down when youth move between levels of care, particularly after hospitalization or crisis episodes. Follow-up providers may not receive timely records, referral pathways may be limited, and families are often left on their own to identify which services exist, which services are available, and which services their insurance will cover. Such care navigation across systems is challenging even for trained professionals. For families dealing with a loved one in mental health crisis or severe needs, or just struggling to navigate and meet their basic needs, these barriers can be insurmountable.
In our discussion, records-sharing was highlighted as a critical barrier by providers. Behavioral health records can be especially difficult to obtain due to privacy requirements, uneven participation in electronic health information systems, and limited technology capacity among smaller providers. Lack of consistent information sharing creates practical barriers for follow-up care after hospitalization, crisis stabilization, or movement between school-based and community-based services. Primary care providers shared that they often see patients referred by mental health providers for follow-up care with little to no information regarding the patients’ previous care received or ongoing care needs.
Prevention and Early Intervention
Awareness of early warning signs is growing among youth-serving adults. However, these efforts remain uneven across the region and are not reaching all youth, especially those outside traditional public school settings. Prevention efforts are strongest when they are embedded in places where youth already spend time, including schools, afterschool programs, libraries, recreation programs, faith-based spaces, and community organizations. Youth outside traditional public schools, including homeschooled youth, charter school students, and youth disengaged from school, may not be reached consistently.
Additionally, social-emotional learning, suicide awareness, and early intervention curricula vary widely across communities and may face political, cultural, or implementation barriers. Parental fear and misinformation around social-emotional learning—often stemming from confusing terminology, lack of curriculum transparency, and fears of ideological indoctrination or psychological overreach—can limit schools’ ability to consistently teach how to regulate emotion, cope with stress and seek support before issues escalate. While almost all parents value children's emotional well-being, the "SEL" label has become a lightning rod for broader political and community distrust.
Truancy was also discussed as an early indicator that should not be missed. School absenteeism can be a signal of family stress, unmet treatment needs, school disengagement, feeling unsafe in the school environment, or broader risks connected to the school-to-prison pipeline.
Youth Engagement and Supportive Spaces
The session highlighted the importance of supportive third spaces where youth can build relationships, participate in meaningful activities, and interact with trusted adults. Youth need safe, consistent, and accessible places to build relationships beyond clinical settings. Schools, nonprofits, libraries, faith-based groups, outdoor recreation programs, mentoring networks, and afterschool programs were discussed as essential parts of the regional youth mental health ecosystem.
Social media—a concept which is increasingly occupying the role as a ‘digital third place’ to the active detriment of physical alternatives—was highlighted as a significant contributor to youth mental health issues. Transportation barriers and limited youth activities can leave young people isolated or dependent on parents for connection, and when in-person connection is limited, social media can become one of the few available spaces for youth interaction, even as excessive or unchecked use may contribute to anxiety, depression, and social comparison.
Phone bans in schools were discussed as supporting tools, and 2025 the NC General Assembly passed House Bill 959, which requires school districts to enact policies to block student access to social media on school-issued devices and networks. And there are multiple proposals and laws at the federal level and in many states to enforce stricter age limits on access to social media platforms, a move that the majority of Americans support. However, it was also recognized that preventing youth intent on accessing social media from doing so is an uphill battle that concerned adults are unlikely to win.
Therefore, it is important that youth are supported by a range of trusted adults, including coaches, teachers, mentors, youth workers, and community health workers, to support early identification and support. Youth Mental Health First Aid was discussed as an important tool for equipping adults who regularly interact with young people.
Social Determinants of Health
Youth mental health was repeatedly framed as inseparable from family and community conditions. Poverty, housing instability, transportation barriers, parental health, adverse childhood experiences, childcare access, and employment opportunities all shape whether youth experience mental health stressors and whether families can access care.
Family-focused interventions, housing supports, and awareness of adverse childhood experiences were highlighted as existing strengths in the region, but the scale of social and economic need is larger than the reach of current interventions. And transportation—especially in WNC’s rural areas—remains a barrier not only to healthcare, but also to employment, education, extracurricular engagement, and supportive peer connection.
It was also noted that stigma and dismissive attitudes toward youth mental health still discourage young people from speaking openly or seeking support. While it is absolutely vital to provide multiple opportunities for youth to access mental health supports in the areas they live, learn, work and play, fear of judgement and social fallout from peers and adults can prevent them from taking advantage of .
Next Steps: What policy options do we have to support youth mental health?
Below are some of the policy considerations that were either shared from the presenters, or that emerged from the group discussion.
Short-Term Policy Levers
Expand restorative justice and mediation programs as alternatives to out-of-school suspension, which actively prevents youth from accessing school-related mental health supports.
Increase out-of-school time programming and community-based youth supports.
Engage primary care providers in integrated behavioral health settings.
Improve childcare infrastructure as a family support and workforce stability strategy.
Address barriers to medical record sharing after hospitalization, crisis care, or transitions between providers.
Support school phone policies in ways that improve classroom focus while avoiding overly punitive approaches.
Longer-Term Policy Levers
Improve Medicaid administrative efficiency for behavioral health providers, especially around billing systems, authorizations, and plan contracting.
Address reimbursement rates to reflect the actual cost of youth behavioral health services and support provider access and sustainability.
Invest in programs that provide support for social drivers of health, such as food security, housing, personal safety, etc. (for example, NC’s Healthy Opportunities Pilot).
Increase investment in school-based behavioral health staffing and compensation, including counselors, psychologists, social workers, nurses, and educator supports.
Strengthen cross-system coordination among schools, social services, juvenile justice, primary care, behavioral health providers, and community organizations.
Subsidize social services infrastructure so county agencies and community partners have the staff capacity to collaborate effectively.
Expand transportation and employment opportunities for youth and young adults, especially in rural communities.
Support legislative and regional investments in teen mental health initiatives.
Learn more
WHC Health Network Resources
To access the full report of this analysis and supporting resources, visit the WNC Health Network Youth Mental Health resource page.
Youth Mental Health Information and Educational Resources
Visit the National Institute of Mental Health’s Child and Adolescent Mental Health website for news, educational and other resources related to youth mental health.
The U.S. Centers for Disease Control and Prevention (CDC) page on adolescent and school mental health also has links to many resources and information sources.
❗️Content Notice ❗️The CDC page currently displays a prominent notice added by the Trump administration expressing the administration's position on gender identity. This notice appears separately from the CDC's mental health content and may be distressing to some readers.
If you or someone you know needs support
The SAMHSA’s National Helplineat 1-800-662-HELP (4357) is a free, confidential, 24/7, 365-day-a-year treatment referral and information service (in English and Spanish) for individuals and families facing mental and/or substance use disorders.
NAMI Western Carolina’s website offers many ways to find support, learn more or get engaged in your community, including information and resources on youth mental health, a support group for Parents and Caregivers of Teens who are struggling with mental health concerns, and opportunities for advocacy that can support.
Disclaimer
This content was developed by the WNC Health Policy Initiative in consultation with people and organizations with connections to the health of people of Western North Carolina. Individual or organizational opinions, findings, conclusions, or recommendations are those of the relevant author(s)/interviewee(s) and do not necessarily reflect the view of the WNC Health Policy Initiative or its host institutions of the University of North Carolina Asheville (UNCA), Mountain Area Health Education Center (MAHEC) or our funders.: U.S. Centers for Disease Control and Prevention (CDC)